Contact Vicki
If you have any questions or would just like more information please don't hesitate to get in touch by clicking the button below and filling out the contact form.
Contact Vicki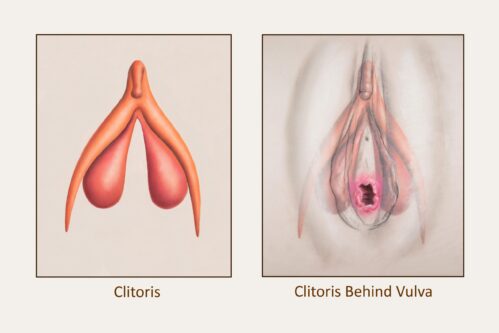
The clitoris and the perineum – the holy grail of womanhood.
We know episiotomy can impact the function and healing of these two sacred parts of the female anatomy, so it is important for women to be educated on what you can do during labour and birth to reduce or eliminate the risk of tearing and decline routine episiotomy.
I’ve been fortunate to spend time at workshops with both Debra Pascali-Bonaro from Orgasmic Birth who shared her 3D clitoris and knitted “pussy puppet” with us and Dr Rachel Reed from Midwife Thinking where we had lots of discussion and shared resources about the clitoris, it was clear that the clitoris is still a mystical part of the female body, so it was valuable learning mixed with knowing smiles.
Do you know what the clitoris looks like?
When I ask my clients most of them say something like “the little G-Spot in the vagina.”
In fact, I’m stunned when some care providers can’t accurately tell me what the clitoris is. I’ve even had a midwife once say that during an episiotomy they don’t go anywhere near the clitoris and that all I was doing was fear mongering, but this again shows a lack of knowledge around the anatomy of the clitoris and the belief that the clitoris is just a “g-spot” and of course, the episiotomy scissors don’t go anywhere near the “g-spot” but the information that I share here will show that episiotomy does in fact damage the clitoris.
So, let’s delve a little deeper – the clitoris is not just that little pea like button at the front junction of the labia minora (inner lips), above the opening of the urethra.
This is in fact the clitoral glans – which is the visible part of the whole clitoris that is very sensitive to touch.
The whole clitoris looks like (for lack of a better description) a chicken wish bone (furcula).
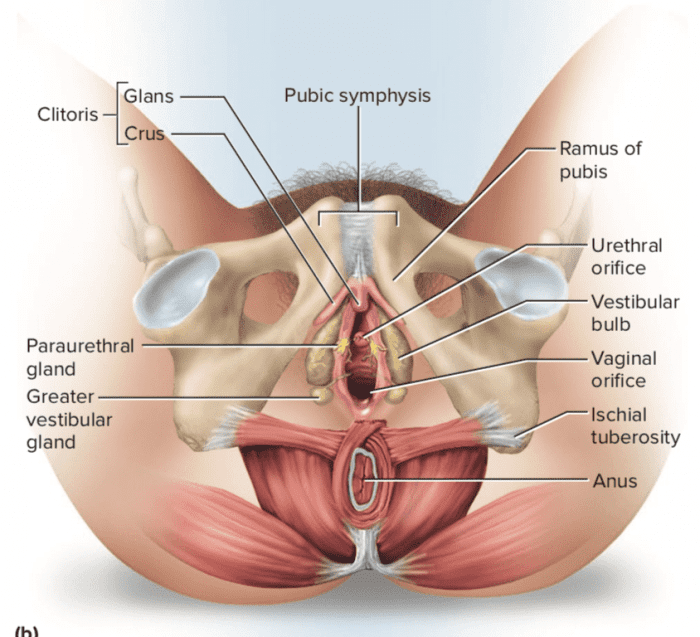
The clitoris is a multi-part system and includes two shafts (called crura), which are around 10cm long that encircle the vagina.
Dr Robert King wrote: “it has at least eighteen distinct interacting functional parts including muscular, erectile, and sensitive tissues.”
MRI studies revealed that most of these structures expand significantly during arousal and the bulbs can effectively wrap around the vagina.
The clitoris is only used for pleasure and there are approximately 8000 nerve endings in the clitoris, whereas men only have 3000 nerve endings in the penis.
We are taught from a young age to disconnect from the pleasure of clitoral stimulation but many women experience orgasm during birth and this is something that should be explored more – how amazing would it feel to experience an orgasmic birth?
Unfortunately, many women who have experienced orgasm during birth keep this to themselves for fear of being shamed or laughed at.
What a long way we have to go in giving women the freedom to express their pleasurable experiences.
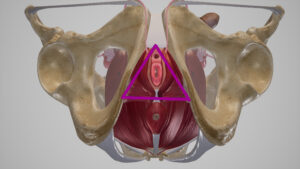
The perineum is the area between the vaginal opening and the anus, and is made up of skin, multiple layers of connective tissue, fatty tissue, muscles and nerves that stretches incredibly as the baby’s head emerges.
The skin covering your perineum contains multiple nerve endings that help with sexual arousal and response.
According to the “Teach Me Anatomy” website: “In clinical practice, the term “perineum” is frequently used to describe the area between the external genitalia and the anus. However, in anatomical terms, the perineum is a diamond-shaped structure. There are two main ways in which the boundaries of the perineum can be described. The anatomical borders refer to its exact bony margins, whilst the surface borders describe the surface anatomy of the perineum.”
(See image above).
https://teachmeanatomy.info/pelvis/areas/perineum/
Many women become fearful about the perineum tearing or needing an episiotomy and wonder how their baby is going to fit through their vagina.
The good news is that a woman is less likely to experience tearing if she is breathing deeply and allowing her body to feel calm and relaxed without tension, relaxing her pelvic floor and going with her own urge to push rather than holding her breathe and being told when to push.
During labour the perineum is amazing and stretches and thins as far as it needs to because it is saturated with the hormone relaxin being released by the receptors in that area.
That is one of the amazing things about being a woman is that our body has been designed to do what it does so beautifully during an undisturbed labour and birth – stretch and open.
If a woman is given the opportunity to birth naturally without being induced or augmented, then her perineum will stretch gradually, slowly and gently the way it has been designed to do and is less likely to experience any trauma.

When the head is crowning the woman may feel a burning type of sensation, but if they are practicing their breathing techniques, then many times that burning is not felt – all women are unique and won’t always have the same experiences.
This burning sensation is like what you would feel if you stretched the corner of your mouth with your fingers – the tissue of the corner of the mouth is similar to that of the perineum.
Try that now – stretch the corner of your mouth until you feel it stretching and “burning” and that is what a woman may experience during childbirth.
Midwives may also reduce the risk of tearing by using warm compresses on the perineum when the head is presenting.
https://www.ncbi.nlm.nih.gov/pubmed/18021143
Here is a video by Professor Hannah Dahlen from University of Western Sydney demonstrating how midwives can prepare and use a warm compress.
https://www.youtube.com/watch?v=_Up-GKAj_fI
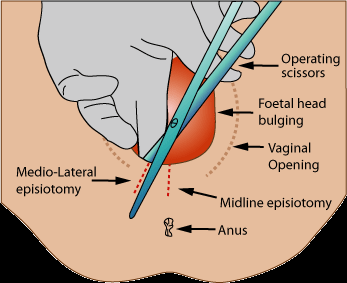
An episiotomy is a surgical cut through the perineum to make the opening larger.
It is done on stretching tissue and muscle and this is very different to an incision that you would have during general surgery.
The medio-lateral episiotomy is cutting through the ipsilateral bulb of the vestibule, which contains thousands of nerves.
A paper by DK Garner et al concluded that for a high (angle ≥45°) mediolateral angle, 100% of cuts impact the bulb of the vestibule (in other words – the clitoris).
For the medium (angle 16-44°) mediolateral angle, the bulb was impacted in 80% of cuts. and for the low (angle 10-15°) mediolateral angle, it was 75%. The midline (angle 0°) does not impact the bulb but has a significantly higher risk of third or fourth degree tearing after the episiotomy is cut. This can lead to fecal incontinence. These investigations occurred in non-crowning circumstances.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7913006/
During birth the perineum is flooded with relaxin and is designed to stretch and with the right position and breathing this reduces the risk of tearing or need for an episiotomy.
There are also oxytocin receptors in the perineum and during an episiotomy these are cut through, which leads to five times increase in a postpartum haemorrhage and could also interfere with breastfeeding.
An episiotomy leads to more pain, longer recover and more sexual dysfunction.
Tears heal better because they are along the muscle lines and not a straight edge.
Ask your Obstetrician what they consider to be a reason for an episiotomy.
Sometimes an episiotomy may be medically necessary, but what we want to avoid is routine episiotomies.
A highly skilled Obstetrician is one who can do an instrumental birth without the necessity for an episiotomy – there are good Obstetricians out there – you just have to ask the right questions.
As mentioned previously, positioning and breathing reduces the risk of tearing.
As Dr Sarah Buckley mentions in her Gentle Birth Gentle Mothering book “nature has a plan” so we should not be interfering with the process.
Research has shown that episiotomies cause more pain, trauma, blood loss, sexual dysfunction and takes longer to heal compared to a natural tear and unless there is a medical need to do an episiotomy then there were no benefits and more harm associated with it.
Yet even though we now have many health bodies advocating for episiotomies to only be conducted when absolutely necessary the episiotomy rate is still high, even in Australia.
https://theconversation.com/episiotomy-during-childbirth-not-just-a-little-snip-36062
https://midwifethinking.com/2018/05/09/the-perineal-bundle-and-midwifery/
An episiotomy is more likely when:
An episiotomy is less likely when:
“An episiotomy does not prevent a tear from occurring, instead it increases the chance of a third- or fourth-degree tear (involving the anal sphincter). A Cochrane Review has summarised the research in this area. Even in obstetric guidelines an episiotomy is not recommended as a way to protect the perineum during birth. Although an episiotomy is easier to suture, a natural tear is less painful and heals quicker. The only excuse for cutting an episiotomy is for an instrumental birth (and not in all cases) or for a baby who needs to be born quickly.
https://midwifethinking.com/2016/01/13/perineal-protectors/
“In women where no instrumental delivery is intended, selective episiotomy policies result in fewer women with severe perineal/vaginal trauma. Other findings, both in the short or long term, provide no clear evidence that selective episiotomy policies results in harm to mother or baby.
The review thus demonstrates that believing that routine episiotomy reduces perineal / vaginal trauma is not justified by current evidence. Further research in women where instrumental delivery is intended may help clarify if routine episiotomy is useful in this particular group. These trials should use better, standardised outcome assessment methods.”
https://www.cochrane.org/CD000081/PREG_selective-versus-routine-use-episiotomy-vaginal-birth
![]()
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4261430
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5558305/
https://theconversation.com/episiotomy-during-childbirth-not-just-a-little-snip-36062
https://pubmed.ncbi.nlm.nih.gov/25610276/
https://file.scirp.org/Html/12-8202761_43131.htm
https://faseb.onlinelibrary.wiley.com/doi/abs/10.1096/fasebj.2018.32.1_supplement.516.4
https://pubmed.ncbi.nlm.nih.gov/16145367/
https://pubmed.ncbi.nlm.nih.gov/27112425/
If you have any questions or would just like more information please don't hesitate to get in touch by clicking the button below and filling out the contact form.
Contact Vicki