Contact Vicki
If you have any questions or would just like more information please don't hesitate to get in touch by clicking the button below and filling out the contact form.
Contact Vicki
Bit of a ranty blog this one about understanding that your cervix should not be on a timer – what we need is for women to go back to basics birthing.
That Friedman’s Curve from the 1950’s has a lot to answer for and is outdated and inappropriate to be used in this day and age and I am aghast that some Obstetricians are still referring to it and putting women on a timer and under pressure and then claiming FAILURE TO PROGRESS (FTP).
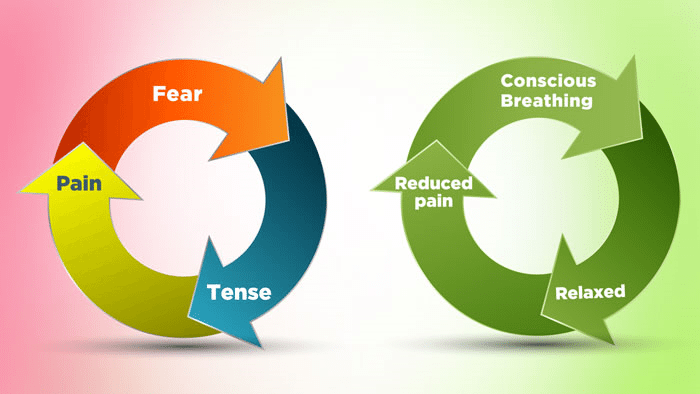
Remember also that FTP stands for FEAR – TENSION – PAIN so if you are not relaxed, calm, feeling safe and doing your breathing then you are not going to be progressing – you are in a “fight of flight” response.
Please do not allow your healthcare providers to convince you that your cervix should be dilating a centimetre an hour.
That is just nonsense – your cervix should not be on a timer.
Interestingly a review published in 2017 by the BJOG – an International Journal of Obstetricians & Gynaecologists stated:
“An expectation of a minimum cervical dilatation threshold of 1 cm/hour throughout the first stage of labour is unrealistic for most healthy nulliparous and parous women. Our findings call into question the universal application of clinical standards that are conceptually based on an expectation of linear labour progress in all women.”
Researcher Dr Sara Wickham suggests, some women may need to go further than the number 10 or be less than 10, and some may even experience what she describes as “cervical recoil” where the cervix actually reduces rather than progresses (in other words you might go from 6cm back to 4cm).
I have seen this happen in some of my own labouring clients, and this can occur when a woman has had her flow of hormones interrupted and she goes into that “fight or flight response” for instinctual safety. This could be where there has been a change of midwife, or a visit from the Obstetrician or just fearful thinking and doubting her body, which then causes her cervix to tighten again.
However, from personal experience as a doula I have also seen women go from being told they are “only” 1cm dilated to then be fully dilated and birthing their baby in less than an hour as well.
CLICK HERE TO GO TO SARA WICKHAM’S WEBSITE
I keep saying to women that you are all unique.
Your pregnancy is unique, your baby is unique, and your birth is unique.
There is no textbook that can cover all that uniqueness.
We can’t put a square peg into a round hole, and we can’t make everyone fit into the same mould.

Keep reminding yourself that it is NOT ABOUT THE CERVIX!
Start asking the question of “WHERE IS BABY” and what are you doing to move baby down further into the pelvis, to put pressure against the cervix to promote dilation?
It really is that simple – yet it is a challenging and labouring part of birth.
If you are yet to birth, make yourself an affirmation poster that says, “WHERE IS BABY – FORGET ABOUT THE CERVIX” and this will be a good reminder for you, but also your healthcare providers as well.
During pregnancy you need to be focusing on how you can create space for your baby to get into a great position – not in a position that is in a textbook or what we have been taught – a position that feels right for them because they don’t go to antenatal classes or read a book, they follow their own instincts.
One of the best ways to prepare your body is by doing the Optimal Maternal Positioning Alignment Protocols. These techniques include using a rebozo to ease tension in the lower back, hips and bottom, the forward leaning inversion, psoas and side lying releases to release the joints and ligaments and create more space. If you find that your labour is not progressing, or baby isn’t in a good position so labour is becoming prolonged or has stalled, then these techniques will help create space, or help baby to reverse out and try again just like you do when you are faced with a roadblock. It definitely won’t be comfortable doing some of these techniques during labour but this could be what helps you avoid a caesarean.
CLICK HERE FOR THE OPTIMAL MATERNAL POSITIONING ALIGNMENT PROTOCOLS
![]()
As a body worker I also encourage my clients to have massage before labour and during labour to release endorphins for pain relief and comfort, but also to loosen any tight muscles.
Get up and move around, do some lunging, squatting, twerking, dancing, crawl around on all fours, and do movements that will help to open the top of the pelvis for baby to get in, and then the bottom of the pelvis to get baby out.
Make it fun and exciting – enjoy your pregnancy, labour and birth and get out of the way your mind has been conditioned that pregnancy, labour and birth is something to be endured. You have grown this baby, nurtured this baby and will birth this baby, so help your baby to feel that energy of love, anticipation and excitement.
On the point of lunging if labour is slow or erratic then I get all my clients doing this during a surge (contraction), which helps to open the outlet of the pelvis, making it easier for baby to get out of the pelvis and this was validated during my OMP Educator training with Ginny Phang-Davey. Obviously if anything you do is painful, then that means to stop.
CLICK HERE FOR THE OMP ARCH BACK SQUAT LUNGE

Like anything there are always going to be exceptions and deviations, and sometimes medical interventions are necessary, but what we need all women to do is take back their power, and ask questions, so that they can make informed choices. If mum and baby are not in danger, and the mum feels she can continue, then women should be given that choice. We want women to do what feels right and good for them – not what is more convenient, easier and faster for their health care providers.
You are only going to have the opportunity to birth this baby once – and only you know what you are prepared to do to have a normal, physiological birth but I do encourage you to do whatever you can to avoid interventions and caesarean – especially that first caesarean if you plan to have more children in the future – because even though we know that “once a caesarean, always a caesarean” is a myth, we also know that once you have a caesarean, your next births are going to be challenging as you navigate through the maternity system that is highly medicalised and not favourable for vaginal birth after caesarean with many care providers.
https://evidencebasedbirth.com/friedmans-curve-and-failure-to-progress-a-leading-cause-of-unplanned-c-sections/
https://midwifethinking.com/2016/06/15/the-anterior-cervical-lip-how-to-ruin-a-perfectly-good-birth/
https://midwifethinking.com/2015/09/09/supporting-womens-instinctive-pushing-behaviour-during-birth/
https://midwifethinking.com/2014/04/16/pushing-leave-it-to-the-experts/
http://www.indybirthservices.com/blog
https://midwifethinking.com/2011/09/14/the-assessment-of-progress/
http://www.sarawickham.com/research-updates/cervical-dilation-is-now-mathematically-shown-to-be-unpredictable/
https://obgyn.onlinelibrary.wiley.com/doi/full/10.1111/1471-0528.14930
http://catalog.nucleusmedicalmedia.com/normal-vaginal-birth-with-cervical-effacement-and-dilatation-dilation/view-item?ItemID=16145
![]()
If you have any questions or would just like more information please don't hesitate to get in touch by clicking the button below and filling out the contact form.
Contact Vicki